High risk patients for surgery include those with compromised cardiac function, previous surgery or irradiation to the neck, a carotid blockage that is difficult to reach by surgical means. In such instances stenting is preferred. Stenting is contraindicated if if there significant renal insufficiency or atherosclerosis of the arch and difficult anatomy
Operator experience with both procedures is critical in reducing complications with either procedure. The major risk during either procedure is stroke which occurs if a fragment of the plaque or clot breaks of and travels to the brain during surgery or stenting. In high volume centers such as Dar Al Fouad Hospital Egypt, the risk of stroke with surgery is 2% or less and with stenting 4% or less.
In either case the best outcomes are achieved by proper procedure selection for each individual patient. It is therefore critical for the patient to seek care by a vascular specialist who is competent in both procedures and unbiased for either technique.
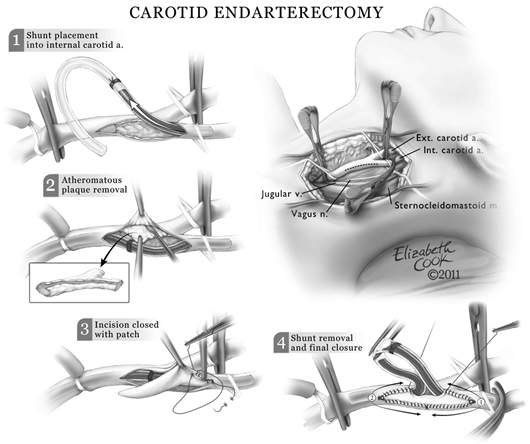
Surgery is commonly performed under general anesthesia and in my practice a temporary shunt is utilized to maintain blood flow to the brain while the carotid artery blockage is being removed ( Fig 5) The procedure can also be performed under regional anesthesia, however this can lead to significant patient anxiety and discomfort.
Stenting is performed under local anesthesia and a protective filter is placed beyond the blockage to capture any particles released from the plaque during deployment of the stent.